
35 Years+ Experience- Best Chiropractor in Decatur GA
(404) 558-4015
- 35 years + experience including orthopedics, physical medicine, physical therapy and neurosurgery
- Participated in the care of 40,000+ patients.
- Video Session - ( Coming Soon )

Some Reviews Of- Best Chiropractor in Decatur, Ga
I am so pleased to have met this wonderful and genuine person. I went to Dr. Castanet after going to numerus PT and chiropractic therapy which did not fix my pain. Dr. Castanet had me fixed and with no pain with in 30 minutes. I simply call it, "magic"! If you are struggling from chronic back pain, I highly recommend trying his method of decompression is the best and safest that I've ever experienced.


Welcome To Backstrong Non Surgical Rehab Clinic
Here at, Backstrong Non-Surgical Rehab Clinic, we have been serving the community of Decatur, GA since 2006. Our main goal is to try provide better, faster treatment for difficult neck and back pain. That’s actually not that difficult to do, but it does require a no-nonsence, expert, experienced approach, with a reduction of red tape. Most spinal problems are not complicated to spine specialists, although the layity is often pooly informed of their problems. I treat many patients who have had ineffective, lengthy treatment, waited too long, paid too much money, and are not well informed of their problem. I’m a no-nonsense guy. I’ll ascertain the problem, tell you what’s the problem, tell you what you should expect, how we will assess success, when you might need a referral to another specialist, and then get you better, faster than other clinics. If not, I will explain what’s next, and refer you to the best alternative provider. Because, in my experience, I have better treatment, I demand that it help you fast, or I find another solution. If you want the fastest track to improvement, I encourage you to test me and my treatment. My experience in medical offices, including orthopedics, physical medicine, physical therapy and neurosurgery means I can provide expert treatment and referral when indicated. We specialize in herniated discs, sciatica, pinched nerves & auto accidents. I’m Dr. Craig Castanet D.C. and I approved this message. I’m the most medically-oriented chiropractor in Decatur GA.
Let’s start with a consultation and find out what you need to get back to living your pain-free life. Call 404-558-4015.







Why Choose Dr. Craig Castanet?
- Specialist in herniated discs, sciatica, pinched nerves, and auto accidents.
- Certifications in many areas of expertise, including Medx rehab, Active release, impairment rating, whiplash and brain traumatology, spinal decompression, functional medicine, functional capacity evaluations, pain management, Spinemed therapy.
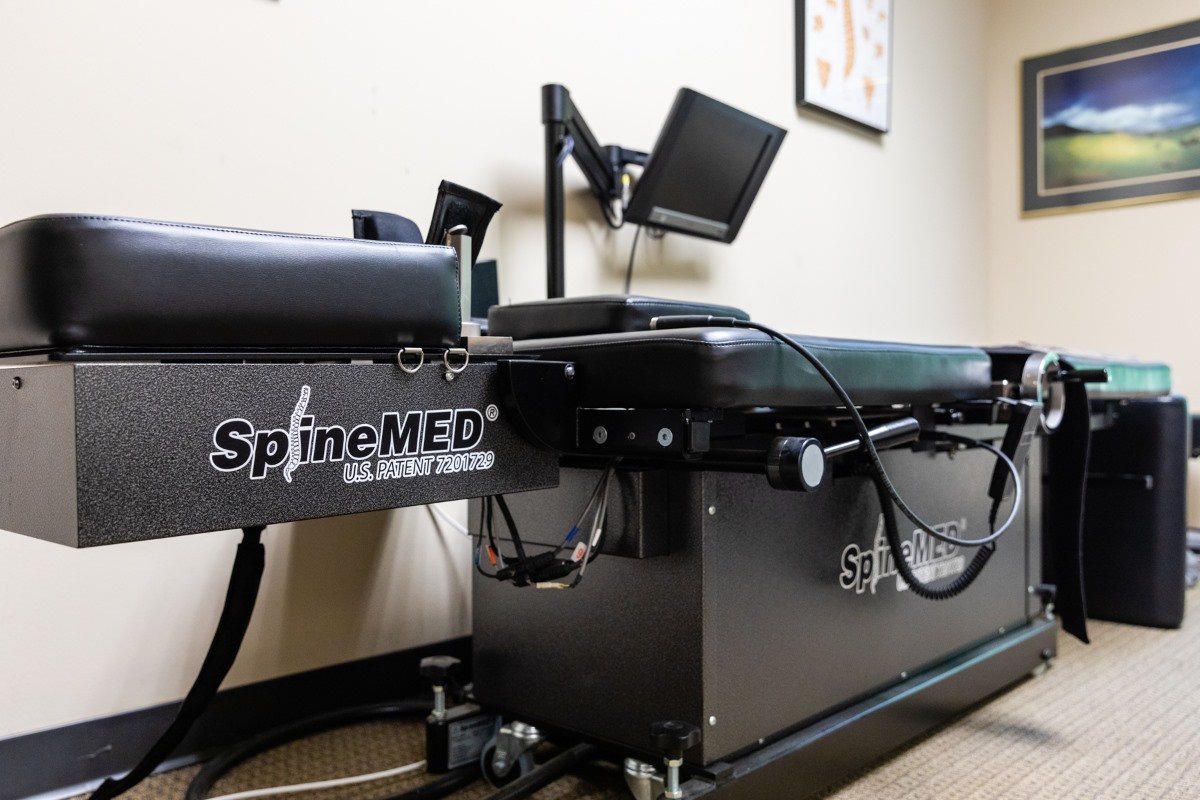
- We are the only clinic in Georgia with SpineMED spinal decompression- the most effective, non-surgical treatment method.
- Previously licensed in California, Florida and Georgia; only practicing in Georgia now.
- Palmer chiropractic graduate; considered by many to be the best chiropractic institution.
Our Services

Spinal Decompression Therapy
Our clinic specializes in spinal decompression therapy. With their expertise and advanced equipment, they offer effective non-surgical solutions for conditions like herniated discs and spinal stenosis. Experience relief from back pain and improve spinal health with spinal decompression therapy at Backstrong in Decatur, GA.
Physical Therapy
Our experienced chiropractor offers top-notch physical therapy services. We provide personalized care and a wide range of treatments to help patients recover from injuries, improve mobility, and achieve optimal physical health. Trust Backstrong for exceptional physical therapy in Decatur, GA.


Car Accident Chiropractor
A car accident chiropractor in Decatur, GA, follows a comprehensive process to assist accident victims. They evaluate injuries, provide personalized treatment plans, and offer pain relief through non-invasive adjustments. With a focus on natural healing and restoring mobility, they support a swift recovery after car accidents.
What Conditions Do We Treat?
Backstrong Non Surgical Rehab Clinic in Decatur GA specializes in Chiropractic, Physical Therapy and Spinal Decompression treatment for neck and back pain arising from herniated discs, pinched nerves, sciatica, joint pain and more, including the Following Conditions
- Sciatica Treatment
- Spinal decompression therapy
- Disc degeneration and Degenerative disc disease treatment
- Herniated disc treatment
- Spinal Stenosis Treatment
- Chiropractor Fibromyalgia
- Scoliosis Treatment
- Neck Pain Treatment
- Bursitis and Tendonitis
- Neuropathy
- Piriformis Syndrome
- Nerve pain and nerve damage relief
- Back spasms
- Neuropathy
- Shoulder pain
- Chronic Lower Back Pain Treatment
- Spondylolisthesis Treatment
- Chiropractor for Sciatica and Sciatic Nerve Pain
- Pinched Nerve Treatment
- Migraine and Headaches
- Arthritis
- Upper Back Pain Relief
How We Take Care of Our Patients?
We provide personalized and compassionate care through individualized treatment plans, patient education, and a range of non-surgical therapies. Our goal is to empower patients to actively participate in their recovery and support them throughout their rehabilitation journey








Best Chiropractor Decatur GA Shares His Experience
Dr. Craig Castanet D.C.
Dr. Craig Castanet graduated from Palmer-West Chiropractic College in 1986. He has 35 years of clinical experience; including 18 years in an orthopedic, physical medicine, and physical therapy clinic, participating in the treatment of more than 40,000 patients. He also dedicated time each week, for 5 years, in a neurosurgical practice, learning surgical indications and procedures. Unlike most chiropractors, he has always had a decidedly “medical orientation”. He has excellent professional relationships with pain physicians, orthopedists, and neurosurgeons because, sometimes, injections and surgery are appropriate.
How To Get To Our Office?
Our Office Facilities
Practice area for our clinic
Frequently Asked Questions
No, you do not need a referral to see a chiropractor. Chiropractors are educated, trained, and considered professionally competent, and responsible, to evaluate any healthcare problem, and treat you, or make an appropriate referral to another healthcare specialist.
I, specifically, worked in orthopedics, physical medicine and physical therapy for 18 years, and spent another 5 years in a neurosurgical practice, part-time, learning surgical indications and procedures. And I make frequent referrals to other healthcare providers, including surgeons, primary care doctors, physical therapists, and pain specialists.
In fact, it is better to see a non-surgical provider first, because surgery is seldom necessary for spinal problems. And if you can find a non-surgical provider that knows a lot about surgical indications and procedures, that is the best case scenario.
This varies widely. My objective is to get patients better or resolved of their pain ASAP. In fact, if patients don’t improve quickly, it is unusual and warrants further consideration. I have treated many patients just once or twice, to their resolution. But that is not the norm. Other times I have treated patients 15-20 times for a certain problem, but that is also unusual. If, however, a patient requires more treatments, it is because they are improving- just slower than usual. Slow progress can be for a variety of reasons. For example, they may have severe spinal degenerative changes.
In my clinical experience since 1987, this newer treatment that I have used since 2006, i.e. spinal decompression treatment, gets more patients better, faster, and longer-lasting, than any other treatment I have seen or used, clinically. It often quickly improves intractable problems that patients have had for years, despite other treatments, from other providers.
Fifty dollars per session. That’s about as much as most people’s co-payments for a spinal specialist.
I will note, as I have in other sections of this website, that Medicare has long decided that spinal decompression treatment is “investigational and experimental”, hence not covered as a service. Conversely, I long ago decided that this superior treatment for neck and back problems would be my focus, because I care about patients, not insurance companies. And I also care about my enthusiasm for practice. Getting patients better is the best part of practice, and I never compromise that objective. My clinical practice is so much improved with this method of treatment, I would not practice without it.
Because this treatment is more effective, that means that the total cost of treatment will be many-fold cheaper than other treatment from chiropractors, physical therapists, pain management and surgeons.
This varies with the severity of the problem. Rarely, for very severe pain, I have treated patients daily, until their pain is much improved. As soon as possible the frequency of treatment for these patients will be reduced, commensurate with their improvement, until resolution.
For more common problems, of moderate severity, patients will often come 2-3 times per week, initially. For less severe pain, you may come once a week or even less frequently. For most patients, once they improve, I will not see them again for many months to several years, until they have another problem, or, perhaps, recurrence of the same problem.
Insurance does not cover spinal decompression treatment. They consider it to be “investigational and experimental”. But since the treatment is no more expensive than most people’s co-payments for a specialist, it doesn’t cost you anymore than other treatments. In fact, it probably costs less, because we don’t bill your insurance company. And, unlike other clinics, most of our patients don’t need to do a great variety of treatments that all get billed separately. Most patients who receive spinal decompression treatement, do not need any other, concurrent form of treatment. That also permits a more critical assessment of the treatment as effective, or not, without introducing confounding variables.
In my estimation, thsi treatment is so effective, it can stand alone, without the need for additional palliative or complementary treatments.
I provide this treatment because it is much more effective, than any other treatment I have used in my professional experience, since 1987.
No. Each profession has its own focus and methods of practice. Medical doctors can prescribe medications and perform surgery, although most are not trained in surgery.
Chiropractors have always specialized in the non-surgical, and non-medication treatment of spinal problems. Many chiropractors also treat the entire body, and some also treat non-musculoskeletal problems.
For example, I am trained in something called functional medicine, which is training in systemic diseases, using labwork evaluation and natural supplements, to resolve and essentially cure disease. Not just manage your disease for profit, but resolve your disease.
Chiropractors vary in their methods of practice. Most are focused on spinal and other musculoskeletal problems. And chiropractors do not want to, nor are they trained, in pharmacotherapy/medications as a means of treatment for patients. Chiropractors, also, are not trained in invasive procedures such as injections and surgery.
Other than that, there is much overlap between chiropractors and musculoskeletal specialist medical doctors. Both doctors use physical medicine procedures as defined in the Current Procedural Terminology manual.
Related Certifications and Training



Gallery - Images & Videos



Our Office Location and Directions
Backstrong Non-Surgical Rehab Clinic
2771 Lawrenceville Hwy #101,
Decatur, GA 30033
Phone: +1 404-558-4015
Monday 8 AM–6 PM
Tuesday 8 AM–6 PM
Wednesday 8 AM–6 PM
Thursday 8 AM–6 PM
Friday 8 AM–6 PM
Saturday Closed
Sunday Closed

